User blogs
Nattokinase, een enzym afkomstig uit gefermenteerde sojabonen (natto), wordt al langere tijd onderzocht vanwege zijn fibrinolytische en vaatondersteunende eigenschappen. In een gerandomiseerde studie (RCT) is de werking van nattokinase (NSK-SD®) bekeken in een Noord-Amerikaanse populatie met een verhoogde bloeddruk. Het blijkt dat door inname van nattokinase de bloeddruk en cardiovasculaire markers verbeterden. Wat werd onderzocht?
Er werden 79 volwassen deelnemers geselecteerd met een verhoogde bloeddruk (≥130/90 mmHg), maar zonder gebruik van medicatie. Ze kregen gedurende 8 weken dagelijks 100 mg nattokinase (2000 FU) of een placebo. Er werd gekeken naar veranderingen in bloeddruk, von Willebrand factor (vWF), renineactiviteit en bloedplaatjesfactor-4. Renine is een enzym dat wordt afgescheiden door de nieren en een sleutelrol speelt in het reguleren van de bloeddruk via het renine-angiotensine-aldosteronsysteem (RAAS). vWF en bloedplaatjesfactor-4 zijn eiwitten die een rol spelen bij de bloedstolling. Significante daling diastolische bloeddruk, verlaging vWF en verbetering renineactiviteit
Na 8 weken liet de nattokinasegroep een significante afname van de diastolische bloeddruk zien ten opzichte van placebo (84 vs. 87 mmHg; p<0,05). Bij vrouwen leidde suppletie met nattokinase tot een verlaging van von Willebrand factor (gemiddeld -26%; p<0,1), een marker geassocieerd met endotheelbeschadiging en verhoogd risico op trombose en beroerte. Daarnaast normaliseerde de renineactiviteit bij deelnemers met aanvankelijk lage waarden (30% van de deelnemers). Hiervan herstelde 66% van de nattokinasegroep naar normale plasmareninewaarden, tegenover slechts 8% in de placebogroep. Conclusie Hoewel het effect op de bloeddruk beperkt is, is het een significant effect ten opzichte van de placebogroep.
Het exacte werkingsmechanisme is nog niet volledig opgehelderd. Maar steeds meer studies (preklinisch en klinisch) wijzen erop dat nattokinase een gunstige invloed kan hebben op de regulatie van de bloeddruk. Meer klinisch onderzoek is nodig om de bevindingen te bevestigen. Referentie Jensen GS et al. Consumption of nattokinase is associated with reduced blood pressure and von Willebrand factor, a cardiovascular risk marker: results from a randomized, double-blind, placebo-controlled, multicenter North American clinical trial. Integr Blood Press Control. 2016;9:95-104.
Copyright (C) Orthokennis https://www.orthokennis.nl/nieuws/nattokinase-verlaagt-bloeddruken-verbetert-cardiovasculaire-markers
https://www.orthokennis.nl/nieuws/nattokinase-verlaagt-bloeddruken-verbetert-cardiovasculaire-markers
PLAY AUDIO here.
Manil Suri and Daniel Morgan are an unusual team: Manil is a mathematics professor and author (of both fiction and nonfiction), while Daniel is a physician and professor of epidemiology, public health, and infectious diseases. But — in what they say is a typical “Smalltimore” moment — both a neighbor and a student had told them they should work together because of a shared interest in false positives on diagnostics tests. The result was a recent First Opinion essay, “Diagnostic tests for rare conditions present a mathematical conundrum,” in which they write about how the more rare a disease ease, the more likely a test will return a false positive.
On this episode of the “First Opinion Podcast,” I spoke with Manil and Daniel about how false positives can cause major problems, how both physicians and patients misunderstand statistics, and how their work plays out in their own lives.
advertisement
Manil imagined a test for a rare condition: “If you tested 20,000 people, only one person would actually have that condition. But remember, if you have a 1% false positive rate, then out of 20,200 people, that is 1% will test positive. And so out of that 200 people, only one person will actually have the disease,” he said. For the other 199, the result may be devastating for no good reason.
Daniel has created a website, TestingWisely.com, where you can learn about how to think through diagnostic testing in a more practical way.
Be sure to sign up for the weekly “First Opinion Podcast” on Apple Podcasts, Spotify, Google Play, or wherever you get your podcasts. And don’t forget to sign up for the First Opinion newsletter to read each week’s best First Opinion essays.
A 5-part docu-series from Holocaust Survivor Vera Sherav is now available in it’s entirety on CHD.TV.
Those….responsible for the pandemic have used two of the weapons that the Nazis used….fear and propaganda.
-Vera Sherav, Holocaust Survivor
You can also watch each section individually:
Part 1: Here We Go Again On Steroids
Part 2: Anyone Who Wants To Start A War Has To Lie
Part 3: Breaking The Veil Of The Real Conspirators
Part 4: This Time Around We’re All Jews
Part 5: Never Give In – Never Give Up
abstract
Systemic mast cell activation disease (MCAD) comprises disorders characterized by an enhanced release of mast cell mediators accompanied by accumulation of dysfunctional mast cells. Demonstration of familial clustering would be an important step towards defining the genetic contribution to the risk of systemic MCAD. The present study aimed to quantify familial aggregation for MCAD and to investigate the variability of clinical and molecular findings (e.g. somatic mutations in KIT) among affected family members in three selected pedigrees. Our data suggest that systemic MCAD pedigrees include more systemic MCAD cases than would be expected by chance, i.e., compared with the prevalence of MCAD in the general population. The prevalence of MCAD suspected by symptom self-report in first-degree relatives of patients with MCAD amounted to approximately 46%, compared to prevalence in the general German population of about 17% (p<0.0001). In three families with a high familial loading of MCAD, the subtype of MCAD and the severity of mediator-related symptoms varied between family members. In addition, genetic alterations detected in KIT were variable, and included mutations at position 816 of the amino acid sequence. In conclusion, our data provide evidence for common familial occurrence of MCAD. Our findings observed in the three pedigrees together with recent reports in the literature suggest that, in familial cases (i.e., in the majority of MCAD), mutated disease-related operator and/or regulator genes could be responsible for the development of somatic mutations in KIT and other proteins important for the regulation of mast cell activity. Accordingly, the immunohistochemically different subtypes of MCAD (i.e. mast cell activation syndrome and systemic mastocytosis) should be more accurately regarded as varying presentations of a common generic root process of mast cell dysfunction, than as distinct diseases.
related article excerpt
More Common Than It Seems
... more
How Massaging Your Calves Can Strengthen Your Heart (4 Easy Exercises)
Heart Health
Etsuko Katahira
Etsuko Katahira
Jun 1 2022
biggersmaller
How Massaging Your Calves Can Strengthen Your Heart (4 Easy Exercises)
Editor’s note: The calves are the driving force behind blood circulation, helping the venous blood flow back to the heart. If the calves are stiff, the blood will not be able to return to the heart. This article introduces four types of massage and exercise methods which use calf movements to help with the smooth flow of blood and body fluids, thus rendering the heart stronger.
Calves are Vascular Pumps to Help Blood Flow Back to the Heart
The blood sent from the heart transports nutrients and oxygen through the blood vessels to the microvasculature throughout the body. During the process, a portion of the blood leaks out of the blood vessels to replenish nutrients for the cells of the subcutaneous tissues and to absorb the waste materials and carbon dioxide, and it then reenters the blood vessels and flows back to the heart. This process takes about 60 seconds, and this cycle will continue as long as the person is alive.
The blood vessels that transport blood from the heart are arteries, and the vessels that return blood to the heart are veins.
The arteries use the heart as a pump, supplying blood at a fixed speed, and the blood flows together to the extremities of the body.
The arteries don’t have to work on their own, as the heart is a pump that helps send blood throughout the body.
So, what is the pump that helps the blood flow from the veins back to the heart? It is the calf muscles.
When the calf muscles are tightened, they will compress the veins that return the blood to the heart from the muscles. You can think of this process as pressing the pump with both hands when filling the tires of a bicycle with air. When standing, the blood in the veins will flow from the bottom to the top, and there are valves inside the veins to prevent backflow.
In modern times, many people don’t have a large physical workload, so they must use some methods to promote the operation of the venous valves to maintain balance.
The following are three methods to massage the calf muscles.
... more
ANALYSIS
New Autopsy Report Reveals Those
Who Died Suddenly Were Likely
Killed by the COVID Vaccine
News Analysis
PREMIUM
December 8, 2022 Updated: December 14, 2022
Dr. Will Jones
New Autopsy Report Reveals Those Who Died Suddenly Were Likely K... https://www.theepochtimes.com/new-autopsy-report-reveals-those-who...
1 of 8 15/12/2022, 09:02
A major new autopsy report has found that three people who died unexpectedly at
home with no pre-existing disease shortly after COVID vaccination were likely
killed by the vaccine. A further two deaths were found to be possibly due to the
vaccine.
The report, published in Clinical Research in Cardiology, the o????cial journal of the
German Cardiac Society, detailed autopsies carried out at Heidelberg University
Hospital in 2021. Led by Thomas Longerich and Peter Schirmacher, it found that in
five deaths that occurred within a week of the first or second dose of vaccination
with Pfizer or Moderna, inflammation of the heart tissue due to an autoimmune
response triggered by the vaccine had likely or possibly caused the death.
Case characteristic of five deaths likely or possibly caused by the COVID vaccines.
New Autopsy Report Reveals Those Who Died Suddenly Were Likely K... https://www.theepochtimes.com/new-autopsy-report-reveals-those-who...
2 of 8 15/12/2022, 09:02
Lymphocyte immune cells (white blood cells) are shown in blue and brown among the heart tissue, causing localised
inflammation that proved fatal.
New Autopsy Report Reveals Those Who Died Suddenly Were Likely K... https://www.theepochtimes.com/new-autopsy-report-reveals-those-who...
3 of 8 15/12/2022, 09:02
In total the report looked at 35 autopsies carried out at the University of Heidelberg
in people who died within 20 days of COVID vaccination, of which 10 were deemed
on examination to be due to a pre-existing illness and not the vaccine. For the
remaining 20, the report did not rule out the vaccine as a cause of death, which Dr.
Schirmacher has confirmed to me is intentional as the autopsy results were
inconclusive. Almost all of the remaining cases were of a cardiovascular cause, as
indicated in the table below from the supplementary materials, where 21 of the 30
deaths are attributed to a cardiovascular cause. One of these is attributed to blood
clots (VITT) from AstraZeneca vaccination (the report was looking specifically at
post-vaccine myocarditis deaths), leaving 20 from other cardiovascular causes.
New Autopsy Report Reveals Those Who Died Suddenly Were Likely K... https://www.theepochtimes.com/new-autopsy-report-reveals-those-who...
4 of 8 15/12/2022, 09:02
For the five deaths in the main report attributed as likely or possibly due to the
vaccines, the authors state:
“All cases lacked significant coronary heart disease, acute or chronic manifestations
of ischaemic heart disease, manifestations of cardiomyopathy or other signs of a
pre-existing, clinically relevant heart disease.”
New Autopsy Report Reveals Those Who Died Suddenly Were Likely K... https://www.theepochtimes.com/new-autopsy-report-reveals-those-who...
5 of 8 15/12/2022, 09:02
This indicates that the authors limited themselves to deaths where there was no
“pre-existing, clinically relevant heart disease,” making the report very conservative
in which deaths it was willing to pin on the vaccines.
Dr. Schirmacher told me:
“We included only cases, in which the constellation was unequivocally clear and no
other cause of death was demonstrable despite all e????orts. We cannot rule out
vaccine e????ects in the other cases, but here we had an alternative potential cause of
death (e.g., myocardial infarction, pulmonary embolism). If there is severe ischemic
cardiomyopathy it is almost impossible to rule out myocarditis e????ects or definitively
rule in inflammatory alterations as due to vaccination. These cases were not
included.
“We did not aim to include or find every case but the characteristics of definitive,
unequivocal cases beyond any doubt. Only by this way you can establish the typical
characteristics; otherwise less strict criteria may lead to ‘contamination’ of the
collective; it is absolutely plausible that by these criteria we may have missed
further cases but the intention of our study was never quantitative or extrapolation
and there are numerous positive and negative bias. But we wanted to establish the
fact not the size.”
It is of course very possible that the vaccines also cause death where there is an
underlying cardiovascular condition, and indeed, that it is more likely to do so.
Thus these five deaths are the minimum from these autopsy cases in which the
vaccines are involved—those in which there is no other plausible explanation.
It is worth noting here that initially in 2021, when the autopsies were first carried
out, Dr. Schirmacher stated that his team had concluded 30–40 percent of the
deaths were due to the vaccines. These earlier estimates may give us a better
indication of how many of the deaths the authors really think are attributable to the
vaccines, when they are unconstrained by highly conservative assumptions (and
looking at causes besides myocarditis). Note that these percentages are based on a
selection of deaths that occurred shortly after vaccination, not a random sample of
all deaths, so the authors rightly warn that no estimation of individual risk can be
made from them.
New Autopsy Report Reveals Those Who Died Suddenly Were Likely K... https://www.theepochtimes.com/new-autopsy-report-reveals-those-who...
6 of 8 15/12/2022, 09:02
Did the autopsies find spike protein from the vaccines present in the heart tissue?
The samples from the five vaccine-attributed deaths were tested for infectious
agents including SARS-CoV-2 (in one instance revealing “low viral copy numbers”
of a herpes virus, which the authors deemed insu????cient to explain the
inflammation). However, no tests were done specifically for the virus spike protein
or nucleocapsid protein, such as have been used successfully in other autopsies to
aid attribution to the vaccine, so unfortunately this evidence was unavailable for
these autopsies.
The autopsies in the report also only cover doses 1 and 2, not any booster doses, and
only deaths within 20 days of vaccination, so the report doesn’t address directly the
question of what’s been causing the elevated heart deaths since the booster rollouts
from autumn 2021 or whether the vaccines can trigger cardiovascular death weeks
or months later. (Other autopsies have confirmed that the spike protein can persist
in the body for weeks or months after vaccination and trigger a fatal autoimmune
attack on the heart.)
What the report does do, however, is establish that people who die suddenly in the
days immediately following vaccination may well have died from a vaccine-related
autoimmune attack on the heart. It also confirms how deadly even mild vaccineinduced
myocarditis can be—and thus why studies like the one from Thailand,
finding cardiovascular adverse e????ects in around a third of teenagers (29.2 percent)
following Pfizer vaccination and subclinical heart inflammation in one in 43 (2.3
percent), and the study from Switzerland finding at least 2.8 percent with
subclinical myocarditis and elevated troponin levels (indicating heart injury) across
all vaccinated people, are so worrying.
The authors of the new study diplomatically write that the “reported incidence” of
myocarditis after vaccination is “low” and the risks of hospitalisation and death
associated with COVID-19 are “stated to be greater than the recorded risk associated
with COVID-19 vaccination”—notably declining to commit themselves to the o????cial
propositions that they dutifully repeat.
The fact that those who die suddenly after vaccination may have died from the
hidden e????ects of the COVID vaccine on their heart is thus now firmly established in
the medical literature. The big remaining question is how often it occurs.
New Autopsy Report Reveals Those Who Died Suddenly Were Likely K... https://www.theepochtimes.com/new-autopsy-report-reveals-those-who...
7 of 8 15/12/2022, 09:02
SSttoopp PPrreessss: Dr. John Campbell has produced a helpful overview of the report’s
findings in his latest video.
Views expressed in this article are the opinions of the author and do not necessarily
reflect the views of The Epoch Times.
New Autopsy Report Reveals Those Who Died Suddenly Were Likely K... https://www.theepochtimes.com/new-autopsy-report-reveals-those-who...
8 of 8 15/12/2022, 09:02
Too big for one blog post.
cont....
Over the following years, Daszak and his Chinese colleague Shi Zhengli, also known as the “bat woman” or “bat lady,” would discover and isolate more than 100 unique coronaviruses all of which, according to Daszak’s own words, can be easily manipulated in the lab.
A copy of a 2015 presentation given by Daszakto the National Academies of Science, Engineering and Medicine showed EcoHealth Alliance’s work in collaboration with the Wuhan Institute of Virology, which was funded by various US agencies. The research involved infections in humanised mice and coronavirus gain-of-function research using human ACE2 receptors, the protein on the surface of a cell to which the SARS-CoV-2 spike protein binds.
 Image compiled from Presentation given by Peter Daszak to the National Academies of Science, Engineering and Medicine
Image compiled from Presentation given by Peter Daszak to the National Academies of Science, Engineering and MedicineShadow Government Architecture: The Vaccine Perspective, NIA Research, 22 August 2022 (timestamp 19:30)
As additional proof of the funding behind his research, at the end of Daszak’s 2011 article, it stated the organisations that funded Daszak and his co-author’s, Dr. Lipkin, research:
Peter Daszak’s work is supported by NIAIDNon-biodefense emerging infectious disease research opportunities award 1 R01 AI079231, an NIH/NSF‘Ecology of Infectious Diseases’ award from the Fogarty International Centre 2R01-TW005869, the Rockefeller Foundation, Google.org, NSF Human and Social Dynamics ‘Agents of Change’ award (SES-HSD-AOC BCS–0826779), and generous support of the American people through the United States Agency for International Development (USAID) Emerging Pandemic Threats PREDICT. The contents are the responsibility of the authors and do not necessarily reflect the views of USAID or the United States Government. Dr. Lipkin’s work is supported bygrants from the National Institutes of Health(AI057158, AI0793231, AI070411, EY017404), Bill and Melinda Gates Foundation, USAID PREDICT, and Defence Threat Reductions Agency. [emphasis our own]
The search for meaning in virus discovery, ScienceDirect, December 2011
In May 2012, the Global Vaccine Action Plan 2011-2020was approved to achieve the Gates Foundation’s “decade of vaccines” vision. The Plan was led by the Gates Foundation, GAVI, WHO, UNICEF, African Leaders Malaria Alliance and the US National Institute of Allergy and Infectious Diseases (“NIAID”).
Further resources:
- Peter Daszak’s prophetic statement to NAS workshop, Totality of Evidence
- Dr. Peter Daszak removed from medical journal’s Covid-19 commission, The Post Millennial, 22 June 2021
- Whistle-blower, Former VP of EcoHealth Partners with Attorney Tom Renz
In 2013, the Technical Advisory Group (“TAG”) on Vaccine-preventable Diseasesreleased a paper from a meeting with the slogan “vaccination a shared responsibility.” The meeting’s objective was to issue recommendations to address the current and future challenges faced by national immunisation programs in the Americas. Part of the 2013 TAG team were representatives from the National Centre for Immunisation and Respiratory Diseases (“NCIRD”), Canada’s Ministry of Health, the Rockefeller Foundation and NIH.
 Shadow Government Architecture: The Vaccine Perspective, NIA Research, 22 August 2022 (timestamp 41:57)
Shadow Government Architecture: The Vaccine Perspective, NIA Research, 22 August 2022 (timestamp 41:57)
Looking at the individuals who signed the 2013 TAG paper, we see the revolving door of individuals moving between three organisations – the Rockefeller Foundation, GAVI and WHO – and national public health bodies.
Anne Schuchat, who signed on behalf of NCIRD, is currently a member of WHO’s Health Hazards Advisory Group and a member of Stanford University’s Global Emerging Infectious Diseases Advisory Committee. Formerly she was a member of GAVI’s board and GAVI’s Programme and Policy Committee and the Audit and Finance Committee. So, she came from GAVI to become a CDC official as director of NCIRD and then became an advisor to WHO.
Arlene King, who signed on behalf of the Ministry of Health of Canada, was a GAVI Alliance board member then she became the Chief Medical Officer of the Ontario Ministry of Health. So, she moved from GAVI to the Canadian government.
Jeanette Vega, who signed on behalf of the Rockefeller Foundation, was a former director of Rockefellers’ National Chilean Public Health Insurance Agency (FONASA). Previously she was a Director at WHO and then was the Vice Minister of Health in Chile. After leaving the Rockefeller Foundation she became a director ofthe National Chilean Public Health Insurance Agency and later Minister of Social Development. So, she moved from WHO to the Chilean government, then to the Rockefeller Foundation and back to the Chilean government.
Roger Glass, who signed on behalf of NIH’s Fogarty International Centre, received the Albert B. Sabin Gold Medal Award in 2015which is awarded by the Sabin Vaccine Institute founded in 1993to continue the work of developing and promoting vaccines. Sabin was best known for developing the oral polio vaccine. In 1934, Sabin conducted research at the Lister Institute for Preventative Medicine, London, and then joined the Rockefeller Institute University.
In 2017, Rajiv Shahwas elected President of the Rockefeller Foundation. Previously he was a director at the Gates Foundation and then he was USAID Administrator under the Obama Administration.
Global Pandemic PreparednessIn May 2018, WHO and the World Bank formed the Global Preparedness Monitoring Board (“GPMB”). In September 2018, the GPMB convened a meeting at WHO in Geneva to discuss key issues on global pandemic preparedness. GPMB had commissioned a study which was spearheaded by the Johns Hopkins Bloomberg School of Public Health. In September 2019, GPMB published a report ‘Preparedness for a High-Impact Respiratory Pathogen Pandemic’.
 Preparedness for a High-Impact Respiratory Pathogen Pandemic, September 2019, pg. 6
Preparedness for a High-Impact Respiratory Pathogen Pandemic, September 2019, pg. 6
The conclusions of the 2019 report included:
 Preparedness for a High-Impact Respiratory Pathogen Pandemic, September 2019, Summary of Conclusions, pg. 11
Preparedness for a High-Impact Respiratory Pathogen Pandemic, September 2019, Summary of Conclusions, pg. 11
 Preparedness for a High-Impact Respiratory Pathogen Pandemic, September 2019, Summary of Conclusions, pg. 13
Preparedness for a High-Impact Respiratory Pathogen Pandemic, September 2019, Summary of Conclusions, pg. 13
The signatories and contributors to the report included HHS’ Rick Bright and Wellcome Trust’s Jeremy Farrar.
 Shadow Government Architecture: The Vaccine Perspective, NIA Research, 22 August 2022 (timestamp 50:28)
Shadow Government Architecture: The Vaccine Perspective, NIA Research, 22 August 2022 (timestamp 50:28)
Before joining the Rockefeller Institute, Rick Brightwas the Deputy Assistant Secretary for Preparedness and Response and the Director of the Biomedical Advanced Research and Development Authority (“BARDA”). He was the “whistle-blower” who fought against hydroxychloroquineas a treatment for Covid. Afterwards, he left government service and is now Chief Executive Officer of the Pandemic Prevention Institute at The Rockefeller Foundation.
To sum up, wealthy organisations and individuals are getting you and your government to pay for and implement private interests through public policies. Policies that are geared towards a pre-determined conclusion that is to the benefit of those wealthy global interests.
Further reading:
- WHO, Bill Gates and Wellcome Trust’s Global Vaccine Fund Lacks Transparency and Accountability
- How Bill Gates & Partners’ money controlled the World’s Draconian Covid Plan
- The Decade of Vaccination: WHO Estimates “Vaccines” Will Reduce the World’s Population by 15%
- Covid Criminal Network Leads to the Gates of Hell
Wealthy investors have created funds and foundations which then engage in various funding activities, while also being responsible for assisting politicians to be elected, or placed, into office. Once the political candidates are in office, they authorise funds to these international organisations to engage in studies, research and “collaborative” efforts.
At the same time, the foundations donate to the international organisations which gives the foundations access to and seems to help them steer the organisations toward certain conclusions.
The image below, using a hypothetical structure, illustrates how this network operates.
 Shadow Government Architecture: The Vaccine Perspective, NIA Research, 22 August 2022 (timestamp 51:57)
Shadow Government Architecture: The Vaccine Perspective, NIA Research, 22 August 2022 (timestamp 51:57)
This vaccine regime structure, as with other shadow government infrastructures, has been built using our money and our elected officials are enabling it. They have weaponised our governments against us.
How do we stop this? One of the solutions is for national governments to stop funding and ban officials’ participation in these international organisations’ activities. And, those officials who have been involved in such activities should submit to a public civilian inquiry.

https://expose-news.com/2022/11/27/shadow-govt-has-built-a-global-vaccine-regime/
 expose-news.com/2022/11/27/shadow-govt-has-built-a-global-vaccine-regimeBy Rhoda WilsonNovember 27, 2022
expose-news.com/2022/11/27/shadow-govt-has-built-a-global-vaccine-regimeBy Rhoda WilsonNovember 27, 2022
The same organisations that have an interest in vaccinations today also had a lot of influence in laying the groundwork decades ago. People tend to think of these large and well-known organisations – such as Rockefeller Foundation, Bill & Melinda Gates Foundation, UNICEF; CDC, GAVI, USAID, the World Bank – as independent of each other, but they are not. They are part of a vaccine infrastructure – a global vaccine regime. Or, as Nations in Actiondescribes it, the vaccine shadow government architecture.
The architecture is headed by wealthy investors who have created funds and foundations which then engage in various funding activities, while also being responsible for assisting politicians to be elected, or placed, into office. At the same time, the foundations donate to international organisations giving the foundations access to and enabling them to steer the organisations toward certain conclusions.
In short, wealthy organisations and individuals are getting you and your government to pay for and implement private interests through public policies. Policies that are geared towards a pre-determined conclusion that is to the benefit of those wealthy interests. ... more
Health & Wellness
![]() COVID-19 much less deadly than previously thought, major study finds
Will Jones
COVID-19 much less deadly than previously thought, major study finds
Will Jones
The Daily Sceptic
Mon, 17 Oct 2022 12:53 UTC
 COVID-19 is much less deadly in the non-elderly population than
previously thought, a major new study of antibody prevalence surveys has
concluded.
COVID-19 is much less deadly in the non-elderly population than
previously thought, a major new study of antibody prevalence surveys has
concluded.
The study was led by Dr. John Ioannidis, Professor of Medicine and
Epidemiology at Stanford University, who famously sounded an early
warning on March 17th 2020 with a widely-read article
in Stat News, presciently arguing that "we are making decisions without
reliable data" and "with lockdowns of months, if not years, life
largely stops, short-term and long-term consequences are entirely
unknown, and billions, not just millions, of lives may be eventually at
stake".
In the new study,
which is currently undergoing peer-review, Prof. Ioannidis and
colleagues found that across 31 national seroprevalence studies in the
pre-vaccination era, the average (median) infection fatality rate of
COVID-19 was estimated to be just 0.035% for people aged 0-59 years and
0.095% for those aged 0-69 years. A further breakdown by age group found
that the average IFR was 0.0003% at 0-19 years, 0.003% at 20-29 years,
0.011% at 30-39 years, 0.035% at 40-49 years, 0.129% at 50-59 years, and
0.501% at 60-69 years.
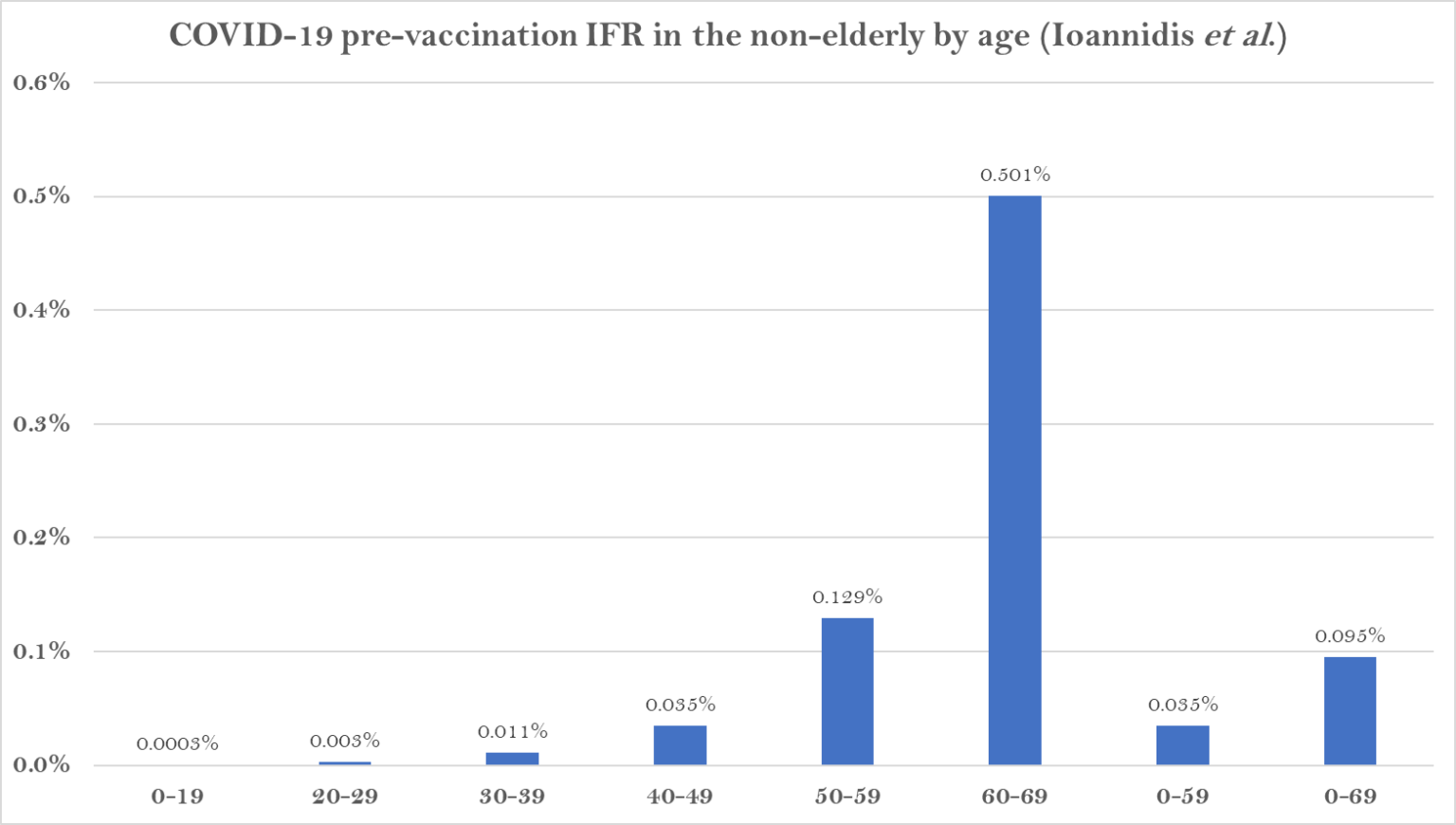 The study states that it shows a "much lower pre-vaccination IFR in non-elderly populations than previously suggested".
The study states that it shows a "much lower pre-vaccination IFR in non-elderly populations than previously suggested".
A breakdown by country reveals the wide range of IFR values across different populations.
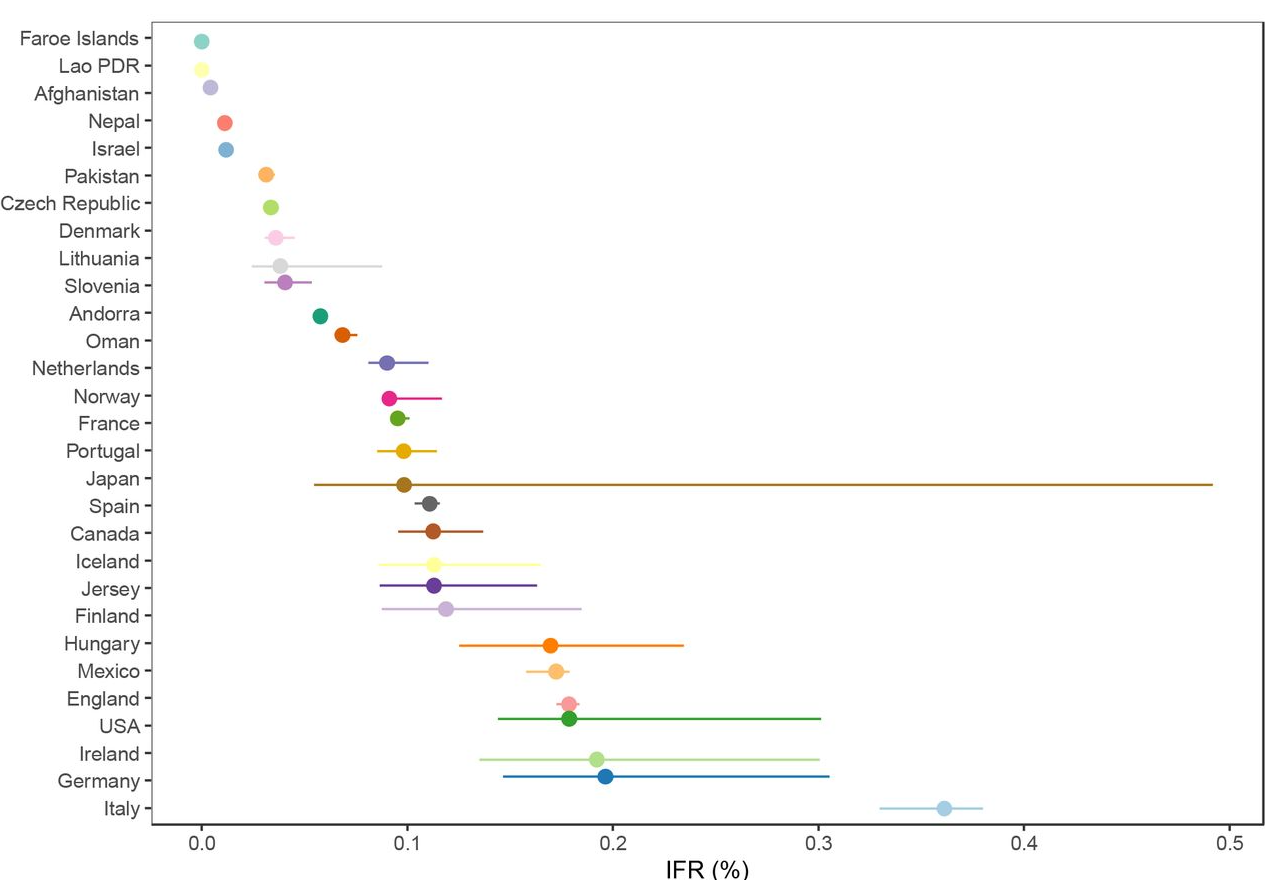 The
significantly higher values for the top seven suggest some of the
difference may be an artefact of, for example, the way Covid deaths are
counted, particularly where excess death levels are similar. Note also
that the antibody studies datefrom various points during the first year of the pandemic, most of them
prior to the large winter wave of 2020-21, when levels of spread and
numbers of deaths were more varied than later in the pandemic as
subsequent waves caused countries to converge.
The
significantly higher values for the top seven suggest some of the
difference may be an artefact of, for example, the way Covid deaths are
counted, particularly where excess death levels are similar. Note also
that the antibody studies datefrom various points during the first year of the pandemic, most of them
prior to the large winter wave of 2020-21, when levels of spread and
numbers of deaths were more varied than later in the pandemic as
subsequent waves caused countries to converge.
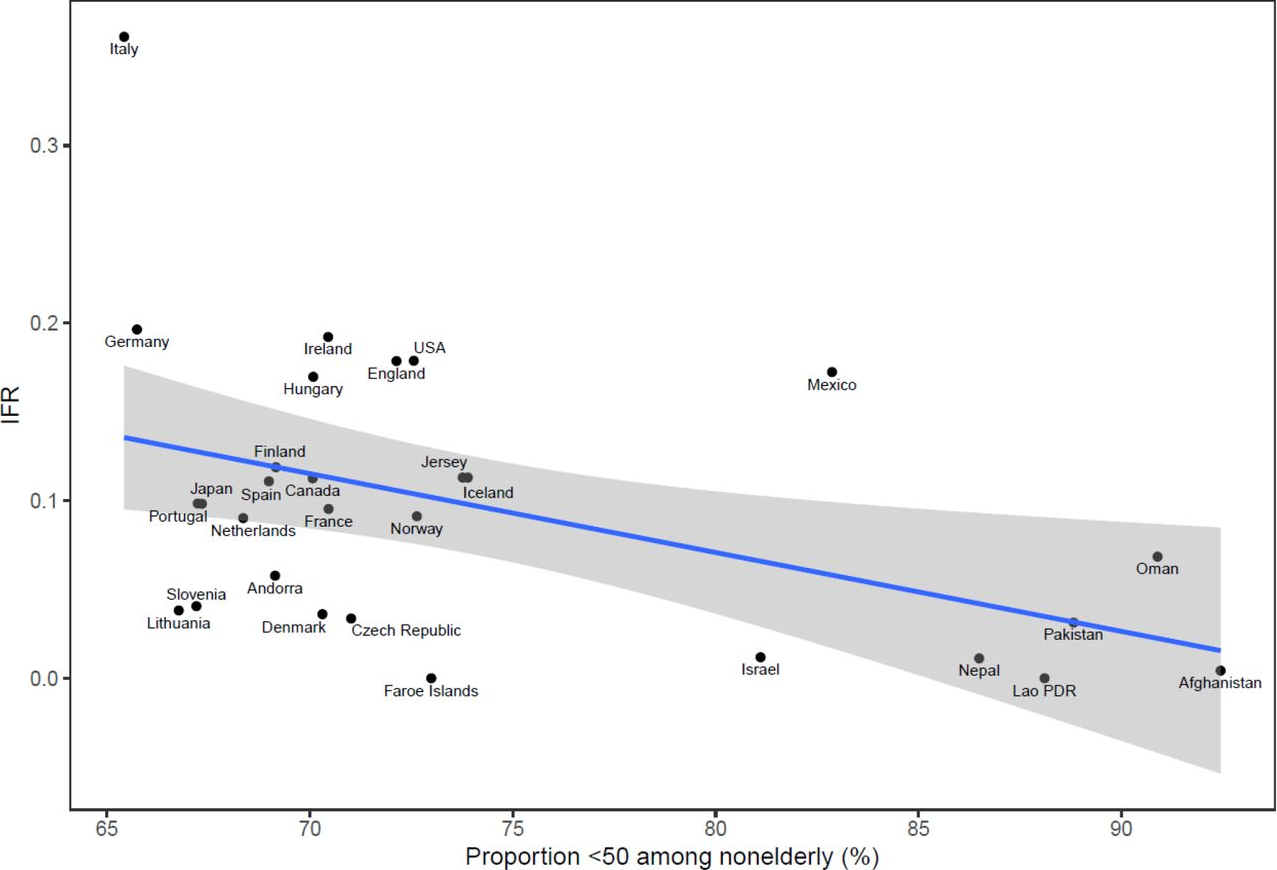
The reason some countries had much lower values and some much higher is
not completely clear. The authors suggest that "much of the diversity in
IFR across countries is explained by differences in age structure", as
per the plot below.
 However,
the age breakdown by country suggests that the IFR differed for each
age group in each country, casting doubt on that suggestion. (In the
chart below, note the logarithmic scale, and ignore the zig-zag lines,
which are due to small countries having low numbers of deaths.)
However,
the age breakdown by country suggests that the IFR differed for each
age group in each country, casting doubt on that suggestion. (In the
chart below, note the logarithmic scale, and ignore the zig-zag lines,
which are due to small countries having low numbers of deaths.)
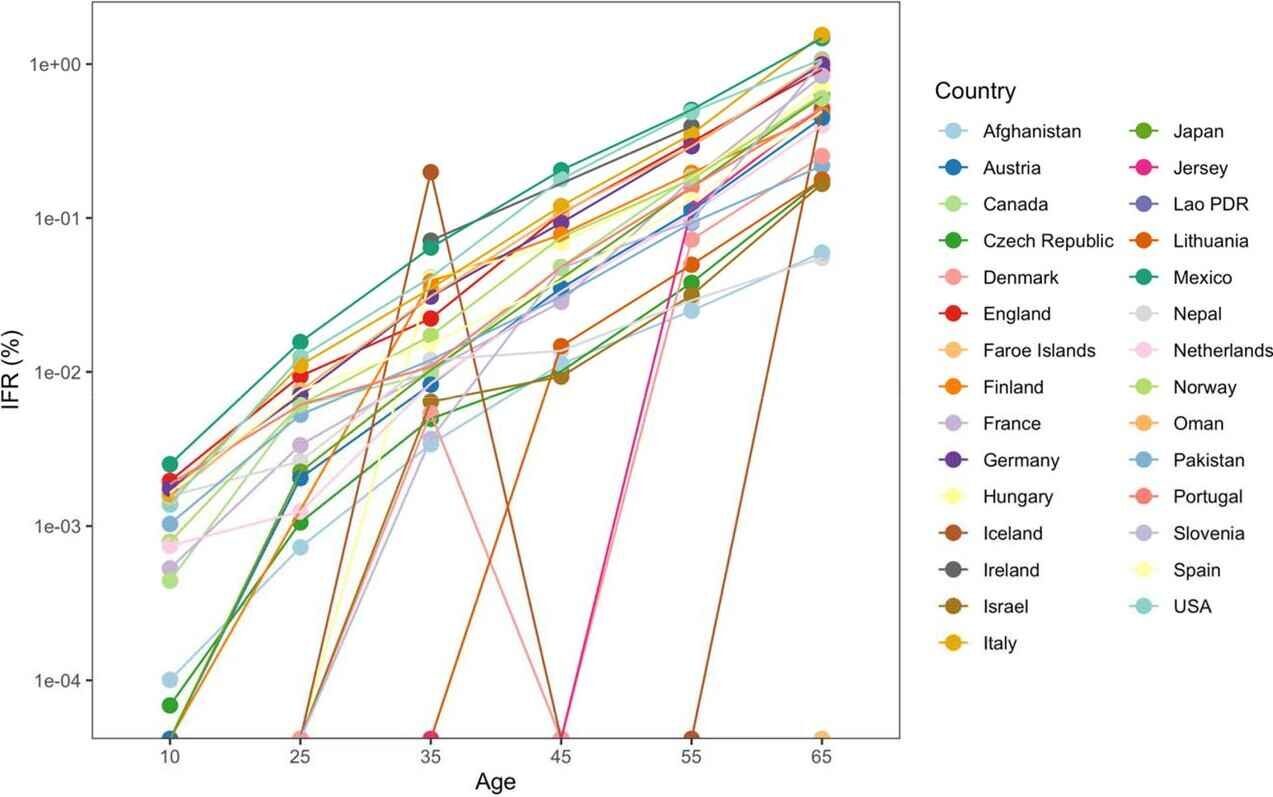 Why
are countries seeing differing IFRs even for the same age groups? The
authors suggest a number of explanations, including data artefacts (e.g.
if the number of deaths or seroprevalence are not accurately measured),
presence and severity of comorbidities (for example, obesity affects
42% of the U.S. population, but the proportion of obese adults is only
2% in Vietnam, 4% in India and under 10% in most African countries,
though it affects almost 40% of South African women), the presence of
frail individuals in nursing homes and differences in management,
healthcare, overall societal support and levels of drug problems.
Why
are countries seeing differing IFRs even for the same age groups? The
authors suggest a number of explanations, including data artefacts (e.g.
if the number of deaths or seroprevalence are not accurately measured),
presence and severity of comorbidities (for example, obesity affects
42% of the U.S. population, but the proportion of obese adults is only
2% in Vietnam, 4% in India and under 10% in most African countries,
though it affects almost 40% of South African women), the presence of
frail individuals in nursing homes and differences in management,
healthcare, overall societal support and levels of drug problems.
Prof. Ioannidis has previously published a number of papers
estimating COVID-19's IFR using seroprevalence surveys. He and his team
conclude that their new estimates provide a baseline from which to
assess further IFR declines following the widespread use of vaccination,
prior infections and evolution of new variants such as Omicron.
Comment: See also:
- John Ioannidis: Another shutdown would do more harm than good
- Modelers were 'astronomically wrong' in COVID-19 predictions, says epidemiologist Dr. John Ioannidis - And the world is paying the price
- Stanford researcher Dr. John Ioannidis says coronavirus might not be as deadly as flu
- Ioannidis releases new medical analysis of 12 global coronavirus studies finding 9 of 12 show COVID-19 fatality rates similar to seasonal flu
- Stanford U. epidemiologist John Ioannidis lambasts the media for panicking the public over Covid-19
- World's leading epidemiologist John Ioannidis on COVID-19 fiasco: 'We are making decisions without reliable data'
Understanding the malinformative nature of pharmaceutical industry propaganda is vital. This article is a good example for analysis. So much of this manipulation of facts, and doublespeak, get blasted at us, that it is worth the time to dissect some of it closely. It helps to know the tricks, so they become easy to spot.
"Stakeholders" have high stakes simultaneously in pharma, insurance, hospitals, retirement funds, media, academia, government policy, and corporations hurt by disability expenses and paying out retirement income for decades per retiree. It is a house of cards because it depends on unaffordable, unsafe, and ineffective medical care.
Pain relief care is ok, but making people healthy is bad for the markets.
===

![]()
View this article online: https://www.claimsjournal.com/news/national/2022/05/18/310515.htm
[bold, italics, and comments by DCforum editor]
Study Links Chiropractic Care to Lower Costs, Faster Return to Work
Chiropractors are involved in only a small fraction of workers’ compensation claims for low back pain in states where insurers or employers control the choice of medical provider, but a report released Tuesday suggests that skepticism [insurance company stakeholder worry?] about runaway costs [of medical sickness care] may be unfounded [thanks to chiropractic care].
A study by the Workers’ Compensation Research Institute found that medical care costs less and claimants return to work more quickly when low back pain treatment is provided solely by chiropractors. Costs were also lower when chiropractors provided physical medicine services but other types of clinicians were in charge of evaluation and management, but the difference was not as dramatic.
“This study will be helpful for policymakers and stakeholders who are interested in re-evaluating the role of chiropractors, especially those who have been adopting evidence-based practices and contributing to cost-effective care,” stated WCRI President and Chief Executive Officer John Ruser in a press release. ... more
