User blogs
PLAY AUDIO here.
Manil Suri and Daniel Morgan are an unusual team: Manil is a mathematics professor and author (of both fiction and nonfiction), while Daniel is a physician and professor of epidemiology, public health, and infectious diseases. But — in what they say is a typical “Smalltimore” moment — both a neighbor and a student had told them they should work together because of a shared interest in false positives on diagnostics tests. The result was a recent First Opinion essay, “Diagnostic tests for rare conditions present a mathematical conundrum,” in which they write about how the more rare a disease ease, the more likely a test will return a false positive.
On this episode of the “First Opinion Podcast,” I spoke with Manil and Daniel about how false positives can cause major problems, how both physicians and patients misunderstand statistics, and how their work plays out in their own lives.
advertisement
Manil imagined a test for a rare condition: “If you tested 20,000 people, only one person would actually have that condition. But remember, if you have a 1% false positive rate, then out of 20,200 people, that is 1% will test positive. And so out of that 200 people, only one person will actually have the disease,” he said. For the other 199, the result may be devastating for no good reason.
Daniel has created a website, TestingWisely.com, where you can learn about how to think through diagnostic testing in a more practical way.
Be sure to sign up for the weekly “First Opinion Podcast” on Apple Podcasts, Spotify, Google Play, or wherever you get your podcasts. And don’t forget to sign up for the First Opinion newsletter to read each week’s best First Opinion essays.
Health & Wellness
![]() COVID-19 much less deadly than previously thought, major study finds
Will Jones
COVID-19 much less deadly than previously thought, major study finds
Will Jones
The Daily Sceptic
Mon, 17 Oct 2022 12:53 UTC
 COVID-19 is much less deadly in the non-elderly population than
previously thought, a major new study of antibody prevalence surveys has
concluded.
COVID-19 is much less deadly in the non-elderly population than
previously thought, a major new study of antibody prevalence surveys has
concluded.
The study was led by Dr. John Ioannidis, Professor of Medicine and
Epidemiology at Stanford University, who famously sounded an early
warning on March 17th 2020 with a widely-read article
in Stat News, presciently arguing that "we are making decisions without
reliable data" and "with lockdowns of months, if not years, life
largely stops, short-term and long-term consequences are entirely
unknown, and billions, not just millions, of lives may be eventually at
stake".
In the new study,
which is currently undergoing peer-review, Prof. Ioannidis and
colleagues found that across 31 national seroprevalence studies in the
pre-vaccination era, the average (median) infection fatality rate of
COVID-19 was estimated to be just 0.035% for people aged 0-59 years and
0.095% for those aged 0-69 years. A further breakdown by age group found
that the average IFR was 0.0003% at 0-19 years, 0.003% at 20-29 years,
0.011% at 30-39 years, 0.035% at 40-49 years, 0.129% at 50-59 years, and
0.501% at 60-69 years.
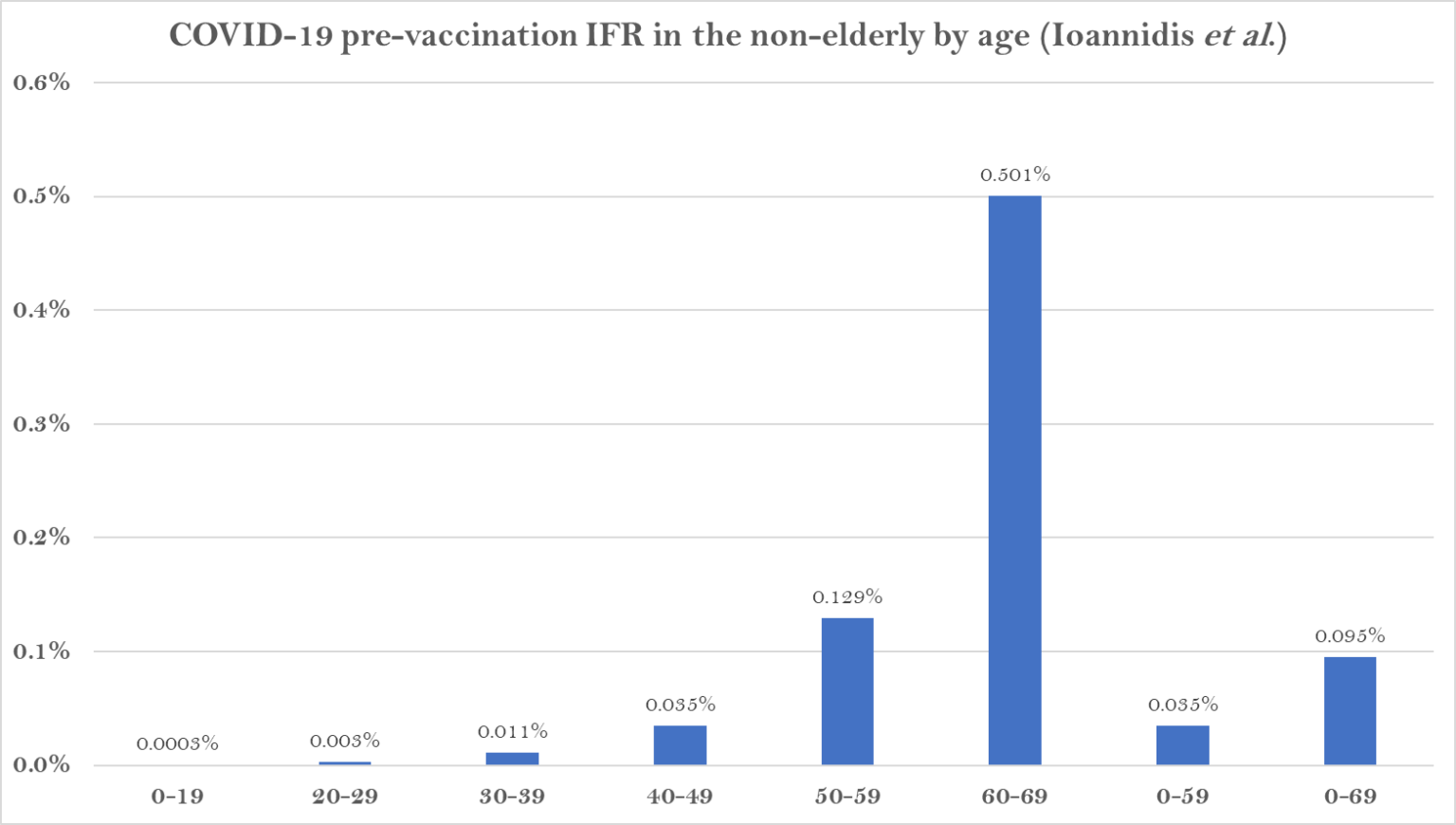 The study states that it shows a "much lower pre-vaccination IFR in non-elderly populations than previously suggested".
The study states that it shows a "much lower pre-vaccination IFR in non-elderly populations than previously suggested".
A breakdown by country reveals the wide range of IFR values across different populations.
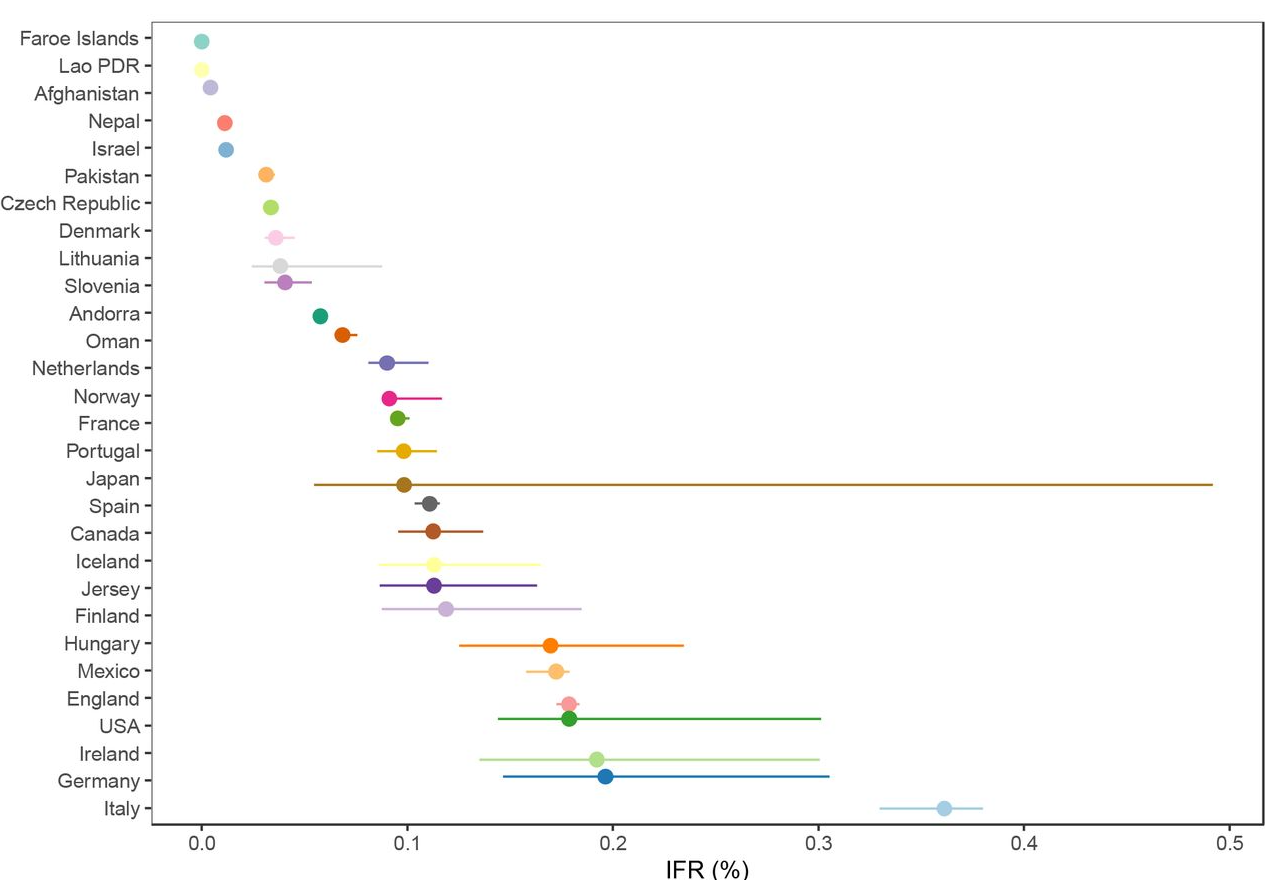 The
significantly higher values for the top seven suggest some of the
difference may be an artefact of, for example, the way Covid deaths are
counted, particularly where excess death levels are similar. Note also
that the antibody studies datefrom various points during the first year of the pandemic, most of them
prior to the large winter wave of 2020-21, when levels of spread and
numbers of deaths were more varied than later in the pandemic as
subsequent waves caused countries to converge.
The
significantly higher values for the top seven suggest some of the
difference may be an artefact of, for example, the way Covid deaths are
counted, particularly where excess death levels are similar. Note also
that the antibody studies datefrom various points during the first year of the pandemic, most of them
prior to the large winter wave of 2020-21, when levels of spread and
numbers of deaths were more varied than later in the pandemic as
subsequent waves caused countries to converge.
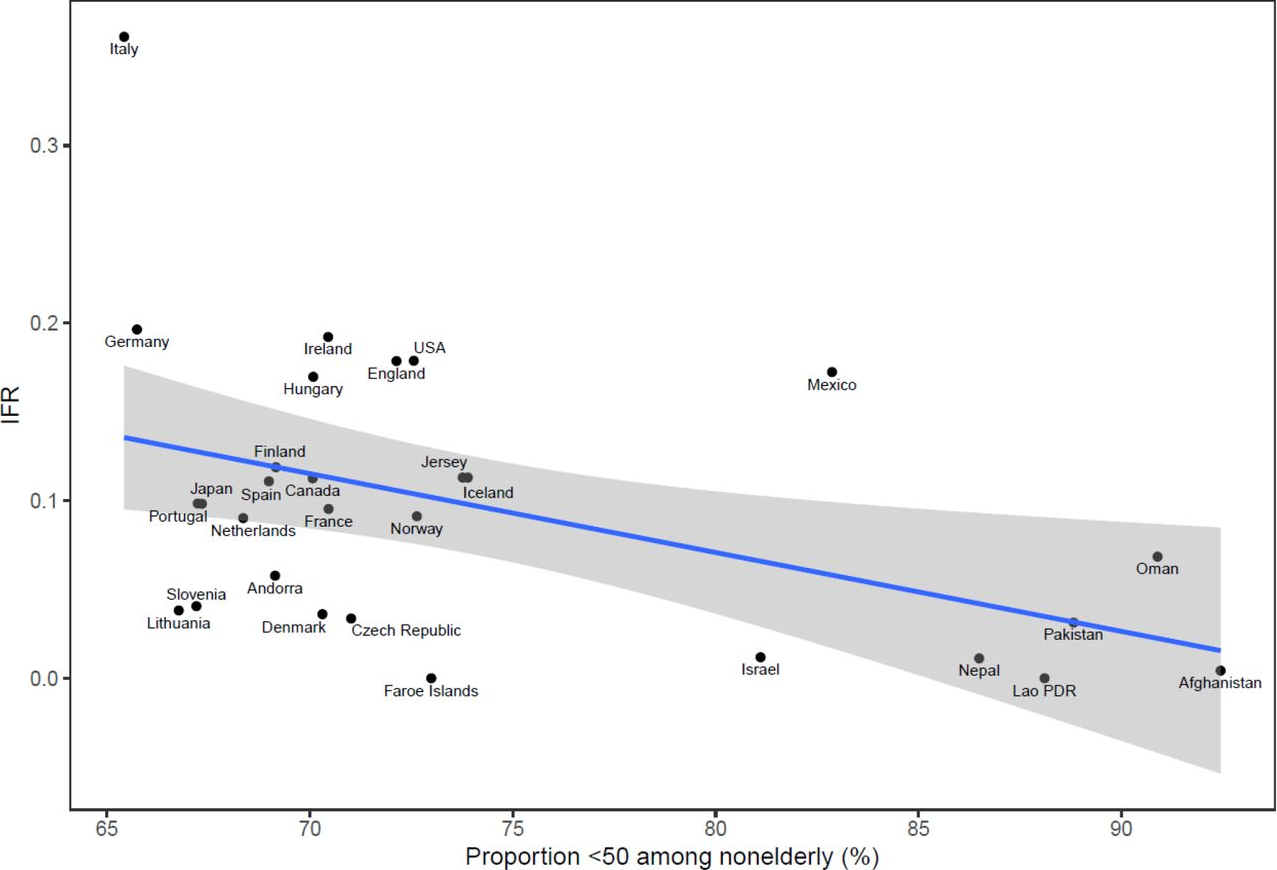
The reason some countries had much lower values and some much higher is
not completely clear. The authors suggest that "much of the diversity in
IFR across countries is explained by differences in age structure", as
per the plot below.
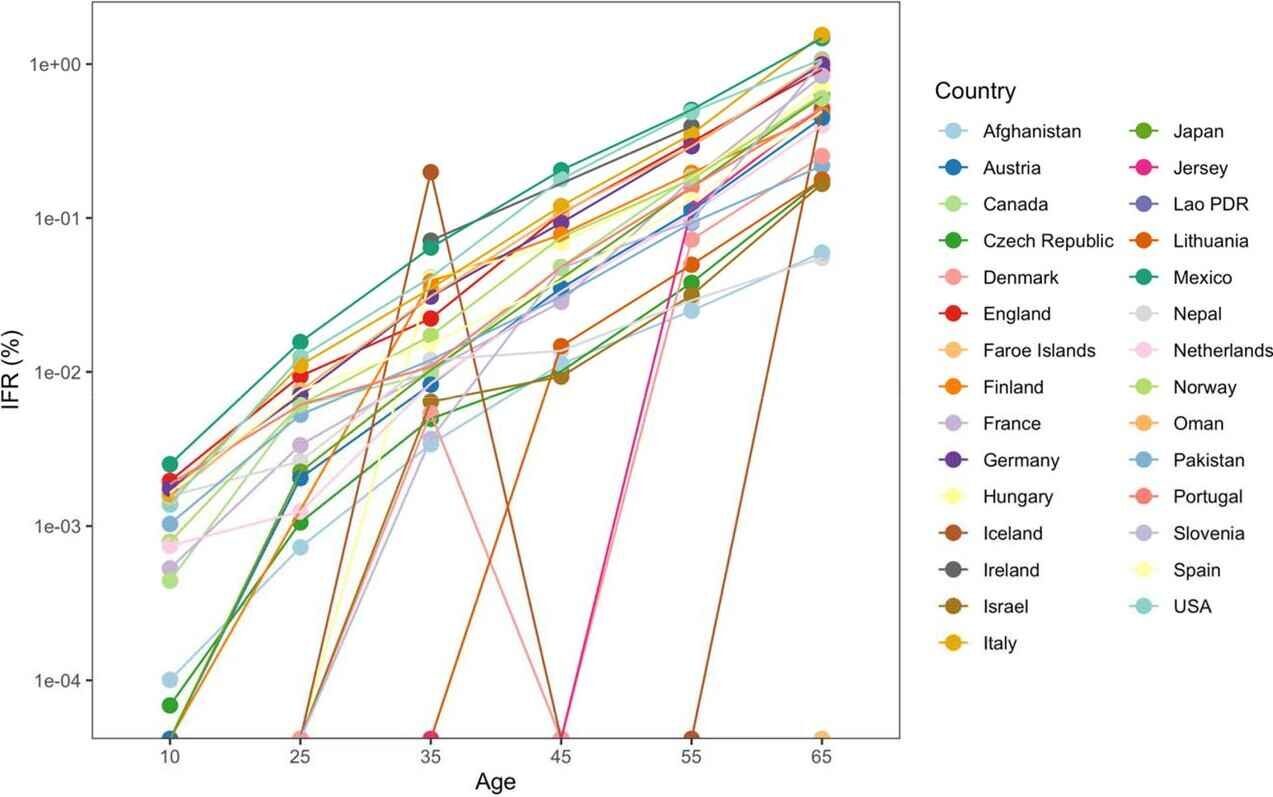
 However,
the age breakdown by country suggests that the IFR differed for each
age group in each country, casting doubt on that suggestion. (In the
chart below, note the logarithmic scale, and ignore the zig-zag lines,
which are due to small countries having low numbers of deaths.)
However,
the age breakdown by country suggests that the IFR differed for each
age group in each country, casting doubt on that suggestion. (In the
chart below, note the logarithmic scale, and ignore the zig-zag lines,
which are due to small countries having low numbers of deaths.)
 Why
are countries seeing differing IFRs even for the same age groups? The
authors suggest a number of explanations, including data artefacts (e.g.
if the number of deaths or seroprevalence are not accurately measured),
presence and severity of comorbidities (for example, obesity affects
42% of the U.S. population, but the proportion of obese adults is only
2% in Vietnam, 4% in India and under 10% in most African countries,
though it affects almost 40% of South African women), the presence of
frail individuals in nursing homes and differences in management,
healthcare, overall societal support and levels of drug problems.
Why
are countries seeing differing IFRs even for the same age groups? The
authors suggest a number of explanations, including data artefacts (e.g.
if the number of deaths or seroprevalence are not accurately measured),
presence and severity of comorbidities (for example, obesity affects
42% of the U.S. population, but the proportion of obese adults is only
2% in Vietnam, 4% in India and under 10% in most African countries,
though it affects almost 40% of South African women), the presence of
frail individuals in nursing homes and differences in management,
healthcare, overall societal support and levels of drug problems.
Prof. Ioannidis has previously published a number of papers
estimating COVID-19's IFR using seroprevalence surveys. He and his team
conclude that their new estimates provide a baseline from which to
assess further IFR declines following the widespread use of vaccination,
prior infections and evolution of new variants such as Omicron.
Comment: See also:
- John Ioannidis: Another shutdown would do more harm than good
- Modelers were 'astronomically wrong' in COVID-19 predictions, says epidemiologist Dr. John Ioannidis - And the world is paying the price
- Stanford researcher Dr. John Ioannidis says coronavirus might not be as deadly as flu
- Ioannidis releases new medical analysis of 12 global coronavirus studies finding 9 of 12 show COVID-19 fatality rates similar to seasonal flu
- Stanford U. epidemiologist John Ioannidis lambasts the media for panicking the public over Covid-19
- World's leading epidemiologist John Ioannidis on COVID-19 fiasco: 'We are making decisions without reliable data'
Evidence based medicine has been corrupted by corporate interests, failed regulation, and commercialisation of academia, argue these authors
The advent of evidence based medicine was a paradigm shift intended to provide a solid scientific foundation for medicine. The validity of this new paradigm, however, depends on reliable data from clinical trials, most of which are conducted by the pharmaceutical industry and reported in the names of senior academics. The release into the public domain of previously confidential pharmaceutical industry documents has given the medical community valuable insight into the degree to which industry sponsored clinical trials are misrepresented.1234 Until this problem is corrected, evidence based medicine will remain an illusion.
The philosophy of critical rationalism, advanced by the philosopher Karl Popper, famously advocated for the integrity of science and its role in an open, democratic society. A science of real integrity would be one in which practitioners are careful not to cling to cherished hypotheses and take seriously the outcome of the most stringent experiments.5 This ideal is, however, threatened by corporations, in which financial interests trump the common good. Medicine is largely dominated by a small number of very large pharmaceutical companies that compete for market share, but are effectively united in their efforts to expanding that market. The short term stimulus to biomedical research because of privatisation has been celebrated by free market champions, but the unintended, long term consequences for medicine have been severe. Scientific progress is thwarted by the ownership of data and knowledge because industry suppresses negative trial results, fails to report adverse events, and does not share raw data with the academic research community. Patients die because of the adverse impact of commercial interests on the research agenda, universities, and regulators.... ... more
Part1: https://www.bitchute.com/video/yII1pZmVYnLN/
PANDA (Pandemics – data and analysis) has been very outspoken with regards to Covid-19, lockdowns and government’s approach to the virus. Their viewpoints have certainly ruffled a few feathers over the past year, with many speaking out against the think tank. Nick Hudson, co-founder of PANDA, spoke at the inaugural BizNews Investment Conference earlier this month.
Part 2: https://www.bitchute.com/video/Pmi2nUhmDool/
More info:
https://www.pandata.org/
https://www.biznews.com/undictated/2021/03/26/nick-hudson-astrazeneca
Source: Philosophers-stone.info Bitchute channel:
https://www.bitchute.com/video/eM5zTvqyPokO/
